Articular cartilage is the smooth, white tissue that covers the ends of bones where they come together to form joints. Healthy cartilage in our joints makes it easier to move. It allows the bones to glide over each other with very little friction.
Articular cartilage can be damaged by injury or normal wear and tear. Because cartilage does not heal itself well, doctors have developed surgical techniques to stimulate the growth of new cartilage. Restoring articular cartilage can relieve pain and allow better function. Most importantly, it can delay or prevent the onset of arthritis.
Surgical techniques to repair damaged cartilage are still evolving. It is hoped that as more is learned about cartilage and the healing response, surgeons will be better able to restore an injured joint.
Cartilage Damage
Hyaline Cartilage
The main component of the joint surface is a special tissue called hyaline cartilage.When it is damaged, the joint surface may no longer be smooth. Moving bones along a tough, damaged joint surface is difficult and causes pain. Damaged cartilage can also lead to arthritis in the joint.
The goal of cartilage restoration procedures is to stimulate new hyaline cartilage growth.
Identifying Cartilage Damage
In many cases, patients who have joint injuries, such as meniscal or ligament tears, will also have cartilage damage. This damage may be hard to diagnose because hyaline cartilage does not contain calcium and cannot be seen on an X-ray.
If other injuries exist with cartilage damage, doctors will address all problems during surgery.
Patient Eligibility

Most candidates for articular cartilage restoration are young adults with a single injury, or lesion. Older patients, or those with many lesions in one joint, are less likely to benefit from the surgery.
The knee is the most common area for cartilage restoration. Ankle and shoulder problems may also be treated.
Surgical Procedures
Many procedures to restore articular cartilage are done arthroscopically. During arthroscopy, your surgeon makes three small, puncture incisions around your joint using an arthroscope.
Some procedures require the surgeon to have more direct access to the affected area. Longer, open incisions are required. Sometimes it is necessary to address other problems in the joint, such as meniscal or ligament tears, when cartilage surgery is done.
In general, recovery from an arthroscopic procedure is quicker and less painful than a traditional, open surgery. Your doctor will discuss the options with you to determine what kind of procedure is right for you.
The most common procedures for cartilage restoration are:
- Microfracture
- Drilling
- Abrasion Arthroplasty
- Autologous Chondrocyte Implantation
- Osteochondral Autograft Transplantation
- Osteochondral Allograft Transplantation
Microfracture
The goal of microfracture is to stimulate the growth of new articular cartilage by creating a new blood supply. A sharp tool called an awl is used to make multiple holes in the joint surface. The holes are made in the bone beneath the cartilage, called subchondral bone. This action creates a healing response. New blood supply can reach the joint surface, bringing with it new cells that will form the new cartilage.
The goal of microfracture is to stimulate the growth of new cartilage by creating a new blood supply.
A sharp tool called an awl is used to make multiple holes in the joint surface. The holes are made in the bone beneath the cartilage, called subchondral bone. This creates a healing response. New blood supply can reach the joint surface. This will bring new cells that will form cartilage.
Microfracture can be done with an arthroscope. The best candidates are young patients with single lesions and healthy subchondral bone.

Drilling
Drilling, like microfracture, stimulates the production of healthy cartilage. Multiple holes are made through the injured area in the subchondral bone with a surgical drill or wire. The subchondral bone is penetrated to create a healing response.
Drilling can be done with an arthroscope. It is less precise than microfracture and the heat of the drill may cause injury to some of the tissues.
Abrasion Arthroplasty
Abrasion arthroplasty is similar to drilling. Instead of drills or wires, high speed burrs are used to remove the damaged cartilage and reach the subchondral bone.
Abrasion arthroplasty can be done with an arthroscope.
Autologous Chondrocyte Implantation (ACI)
ACI is a two-step procedure. New cartilage cells are grown and then implanted in the cartilage defect.
First, healthy cartilage tissue is removed from a non-weightbearing area of the bone. This step is done as an arthroscopic procedure. The tissue which contains healthy cartilage cells, or chondrocytes, is then sent to the laboratory. The cells are cultured and increase in number over a 3- to 5-week period.
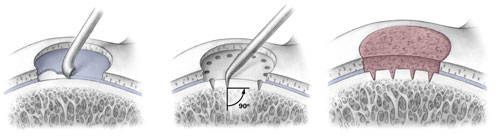
An open surgical procedure, or arthrotomy, is then done to implant the newly grown cells. The cartilage defect is prepared. A layer of bone-lining tissue, called periosteum, is sewn over the area. This cover is sealed with fibrin glue. The newly grown cells are then injected into the defect under the periosteal cover.
ACI is most useful for younger patients who have single defects larger than 2 cm in diameter. ACI has the advantage of using the patient’s own cells, so there is no danger of a patient rejecting the tissue. It does have the disadvantage of being a two-stage procedure that requires an open incision. It also takes several weeks to complete.
Osteochondral Autograft Transplantation
In osteochondral autograft transplantation, cartilage is transferred from one part of the joint to another. Healthy cartilage tissue – a graft — is taken from an area of the bone that does not carry weight (non-weightbearing). The graft is taken as a cylindrical plug of cartilage and subchondral bone. It is then matched to the surface area of the defect and impacted into place. This leaves a smooth cartilage surface in the joint.
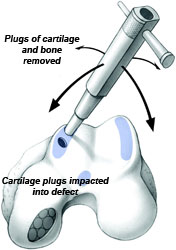
A single plug of cartilage may be taken or a procedure using multiple plugs, called mosaicplasty, may be performed.
A single plug of cartilage may be transferred or a procedure with multiple plugs, called mosaicplasty, may be done.
Osteochondral autograft is used for smaller cartilage defects. This is because the healthy graft tissue can only be taken from a limited area of the same joint. It can be done with an arthroscope.
Osteochondral Allograft Transplantation
If a cartilage defect is too large for an autograft, an allograft may be considered. An allograft is a tissue graft taken from a cadaver donor. Like an autograft, it is a block of cartilage and bone. In the laboratory it is sterilized and prepared. It is tested for any possible disease transmission.
An allograft is typically larger than an autograft. It can be shaped to fit the exact contour of the defect and then press fit into place.
Allografts are typically done through an open incision.
Stem Cells and Tissue Engineering
Current research focuses on new ways to make the body grow healthy cartilage tissue. This is called tissue engineering. Growth factors that stimulate new tissue may be isolated and used to induce new cartilage formation.
The use of mesenchymal stem cells is also being investigated. Mesenchymal stem cells are basic human cells obtained from living human tissue, such as bone marrow. When stem cells are placed in a specific environment, they can give rise to cells that are similar to the host tissue.
The hope is that stem cells placed near a damaged joint surface will stimulate hyaline cartilage growth.
Tissue engineering procedures are still at an experimental stage. Most tissue engineering is performed at research centers as part of clinical trials.
Rehabilitation
After surgery, the joint surface must be protected while the cartilage heals. If the procedure was done on your knee or ankle, you may not be able to put weight on the affected leg. You will need to use crutches to move around for the first few weeks after surgery.
Your doctor may prescribe physical therapy. This will help restore mobility to the affected joint. During the first weeks after surgery, you may begin continuous passive motion therapy. A continuous passive motion machine constantly moves the joint through a controlled range of motion.
As healing progresses, your therapy will focus on strengthening the joint and the muscles that support it. It may be several months before you can safely return to sports activity.